Defining Vitreoretinal Lymphoma
- Contents:
Vitreous Biopsy for VRL
Any 20-25G vitreous cutters can collect vitreous humor for a vitreous biopsy, although a larger diameter is less likely to destroy the lymphoma cells. First, the right-hand vitreous cutter is inserted into the eye. The cutter is then rotated to collect at least 1 mL of the undiluted vitreous humor while gradually compressing the eyeball with a cotton swab under no perfusion to maintain intraocular pressure. The cut rate of the vitreous cutter is set to a low level (400-800 rpm) to reduce cell destruction, and a 5-10 mL disposable syringe is attached to the suction tube of the vitreous cutter. After conducting sufficient amounts of aspiration, the vitreous cutter is removed from the eye while maintaining the pressure on the eye. The intraocular irrigation line will then be opened to start intraocular irrigation, and the intraocular pressure will slowly be decreased. If the pressure is released too early, there is a risk of ectopic hemorrhage occurring in the eye from ocular collapse. The vitreous humor that accumulated in the aspiration tube will also be removed into a disposable syringe and submitted as an undiluted sample.
The vitrectomy is then continued with the intraocular perfusion activated. A high cut rate (2,500 rpm) is acceptable. At the end of the surgery, the waste fluid (40-80 mL) collected in the waste cassette is submitted for examination as a diluted vitreous humor sample. The undiluted vitreous sample is used for cytological diagnosis and IL-10/IL-6 concentration ratio measurements.
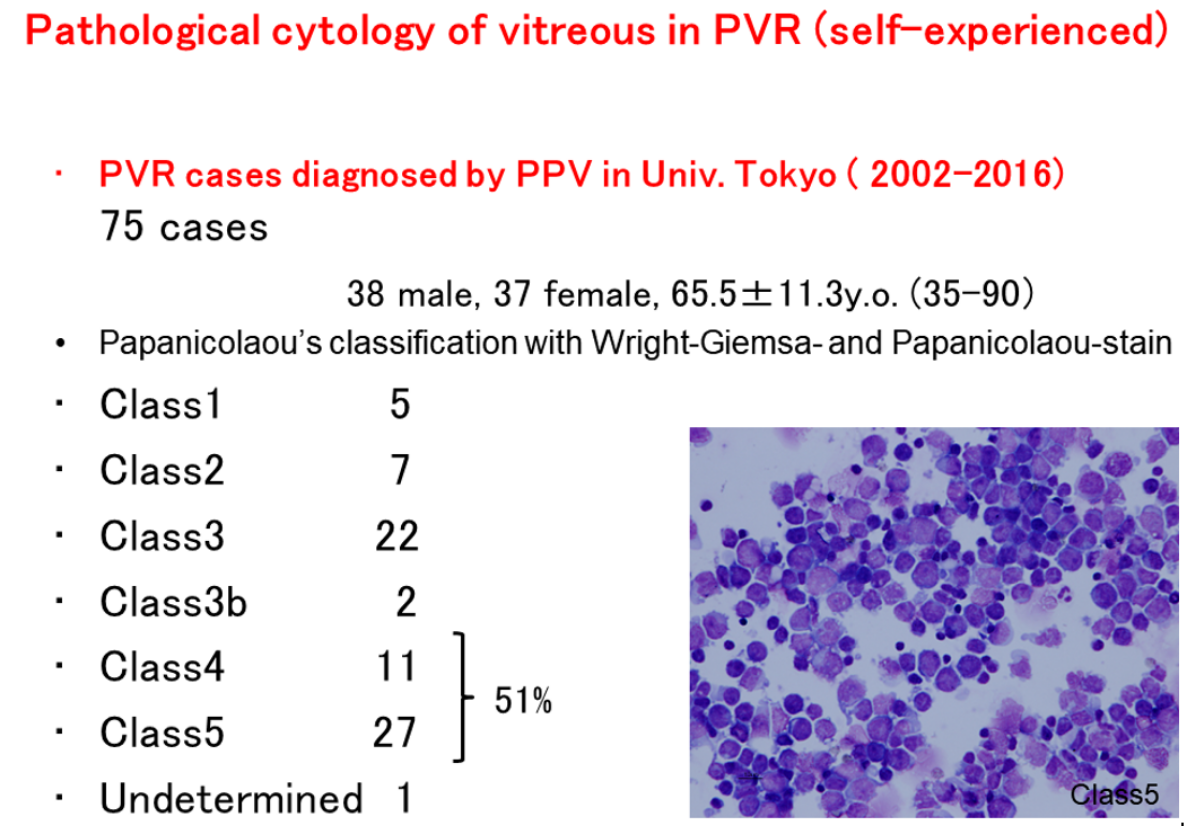
In general, cytological and histopathological diagnoses classify class 4 or higher as malignancy. As the vitreous humor of VRL contains not only lymphoma cells, but also a large number of reactive lymphocytes that migrated into the vitreous body due to inflammatory reactions, only 30% of the cases can be diagnosed with solely a cytological diagnosis. Although international diagnostic criteria for VRL are not standardized, positive cytology and histopathology are conducted as the basis for diagnosis, and tests such as IL-10/IL-6 (>1), IgH gene rearrangement (positive), and B-cell lymphoma phenotype (positive) by flow cytometry are also performed. Experts often diagnose VRL when multiple of these diagnosis methods test positive.
A standard treatment against VRL has not yet been developed, and national guidelines from the Japanese Society of Hematology and Japanese Ophthalmological Society nor international guidelines from NCCN yet exist. Ocular treatment includes radiotherapy and methotrexate (MTX) injections. Combinations of ocular therapy, chemotherapy, and whole-brain radiotherapy have been clinically trialed, but no standard treatment has been set.